Case for iPhone – IBOOLO
People May Ask
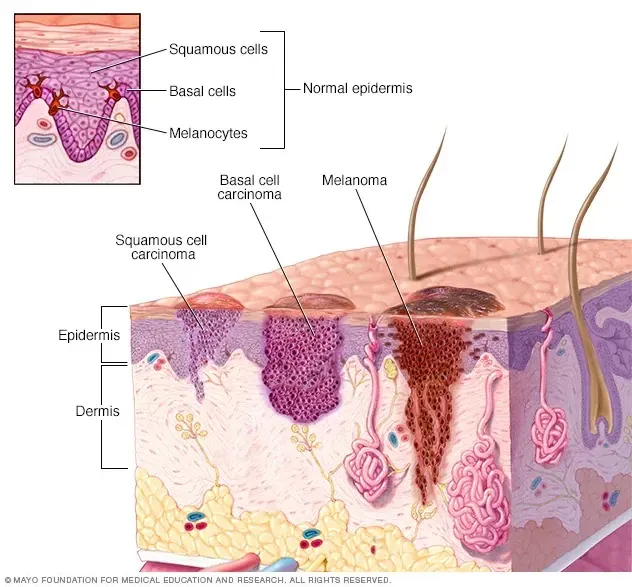
A melanocytic nevus, medically referred to, signifies a mole that can manifest itself anywhere across the human body. These nevi are considered benign in nature, meaning they are non-cancerous and generally necessitate no form of therapeutic intervention. However, it is noteworthy that a minute fraction of melanocytic nevi may undergo a transformation, leading to the development of melanoma within their structure.
Yet, the presence of dysplastic nevi poses a significant threat to the development of melanoma, with an individual's risk escalating proportionately to the number of such nevi they possess (1, 3). According to investigative studies, individuals harboring more than five dysplastic nevi are estimated to have a melanoma risk approximately tenfold higher compared to those without any such nevi.
Both Spitzoid melanoma and Spitz nevus exhibit similar visual characteristics. Nevertheless, the former is a form of malignancy. Cancerous cells proliferate without restraint and have the potential to disseminate to other bodily regions. Conversely, a Spitz nevus represents a benign skin lesion, typically appearing pink or red, contrasting with the brown or black hue of other nevi.
Explosive melanocytic nevi (EMNs) encompass the abrupt emergence of cutaneous nevi spanning several weeks to months. This phenomenon commonly manifests in young adult individuals and can be attributed to a myriad of potential underlying factors.
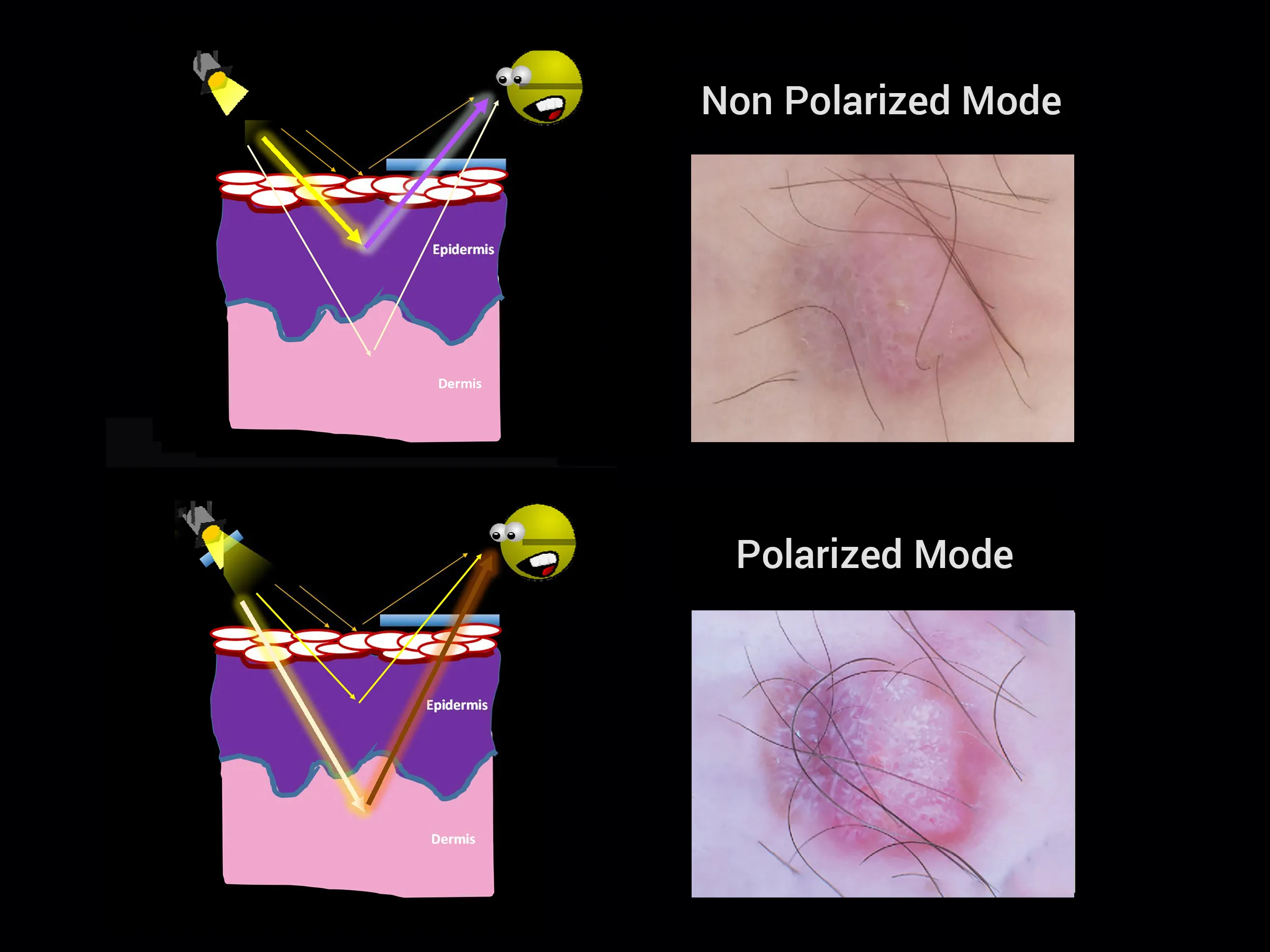
Generally, upon dermatoscopic examination of a dermatofibroma, one can observe a subtle interlacing pattern or a simulated network encompassing a light, non-distinctive region. On occasion, the central lighter region may exhibit white streaks and brown voids, forming a so-called "negative network." Moreover, during polarized dermoscopy of dermatofibroma, crystalline formations, often manifesting as white, lustrous lines, are frequently observed.